1
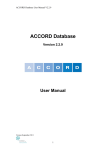
UNC Health Registry Data Source Documentation TableofContents i.HealthRegistryDataCollectionOverview...............................................................................2 Section1:TrackingStudyEvents.....................................................................................................3 Section2:Enrollment..........................................................................................................................7 Section3:Biospecimens.....................................................................................................................8 BiospecimenProcessFacility–BloodSamples.....................................................................................8 TissueProcurementFacility–Tissue........................................................................................................9 Section4:Questionnaires................................................................................................................10 EnrollmentQuestionnaire..........................................................................................................................10 BaselineQuestionnaire(CDART).............................................................................................................10 Cancer‐SpecificQuestionnaires(CDART).............................................................................................10 AnnualFollow‐up(CDART)........................................................................................................................11 Section5:MedicalRecordsAbstraction......................................................................................12 CDW‐HBillingCodes–CancerSpecificQuestionnaireAssignment............................................12 AbstractedMedicalRecordDataElements..........................................................................................13 MedicalRecordHand‐Abstraction..........................................................................................................15 Appendix1.System‐SpecificInformation..................................................................................17 PatientTrackingSystem.............................................................................................................................17 OverviewofBSPLIMSQualityAssurance/QualityControl..........................................................18 BioSpecimenFacilityInformationTechnologies(LIMS).................................................................20 FutureTPFLIMSSystem..............................................................................................................................21 ElectronicRegistrySystem(ERS).............................................................................................................21 Appendix2.System‐SpecificDataMappings.............................................................................23 CPR‐ORTissueCollectionTracking.....................................................................................................................23 i. Health Registry Data Collection Overview Figure1–StagesofDataCollection Section 1: Tracking Study Events Withalargeandcomplexstudy,ensuringaproscribedsequenceofeventsrequires operationalsystemsthataccuratelyandregularlyrecordsubjectstatussothatthenext eventcanbeascertainedandfutureworkloadsbedetermined. SubjectsenrolledintheUNCHealthRegistrycantakeavarietyoftrajectoriesthrough studyeventsdependingondateofenrollment,specificcancertype,andlengthoffollow‐up. Trackingprogressthroughstudyparticipationeventsrequiresasystemforloggingthe sequenceofeventsforeachindividual. Uponasubject’senrollmentintothestudyinthehospital(RecruitmentSchedule SuccessfulConsentEnrollment)theybecomeeligibletoreceivethetelephone‐based baselinequestionnaire.Ascancer‐specificbillingcodesaregeneratedduringvisitstoUNC Hospitals,thetrackingsystemautomaticallymatchescodesthattriggercancer‐specific questionnaires. Interviewerdashboard,patientlookup,schedulingofinterviews,andcancer‐specific questionnairearekeyfeaturesofthesysteminterface.Additionally,thesystemisusedfor generationofpatientcontactmaterialsandisakeyadministrativeinterface,andisa methodforloadingsubject‐specificstudyconsentandHIPAAdocuments.Theinterfacealso providesstaffwithawaytorecordandverifyasubject’svital/deathstatus. DetailsonthespecificuseofthestudytrackingsystemaredetailedintheInterviewer ProtocolDocument. Screenshots Figure2.PaTSyHomeScreen.ThisdashboardprovidessummaryinformationonInterviewStatus,ThankYou letters,andAncillaryStudyTasks Figure3.PatientSummaryPage‐ContainscontactanddemographicinformationandlinkstoInformedConsent anHIPAADocuments Figure4.PatientContactInformationandCallLog Figure5.ParticipantEventStatusPage.SpecificInformationonEventsandCancer‐SpecificInterview. Figure6.ICD‐9EntryScreen.Cancer‐specificICD‐9Codestriggerspecificquestionnaires. Figure7.InterviewerAppointmentQueue.TheHotListindicatesinterviewsscheduledforthecurrentday,while theQueuelistsindividualswithanoutstandinginterviewstatus. Section 2: Enrollment EnrollmentintotheHealthRegistryoccurswhenanindividualisdeemedtobeeligible basedonclinicscheduledata,isapproachedbyahealthregistryrecruiter,andinformed consentisprovidedbythepatientafterlearningabouttherisksandbenefitsof participation. Theenrollmentprocessbeginswithalistofeligibleindividualsvisitingcancerclinicsatthe NCCancerHospitaleachday.ClinicscheduledataisobtainedfromUNCHealthcare appointmentschedulingsystemsthroughtheCarolinaDataWarehouseforHealth(CDW‐ H)andispreparedonadailybasis. Theclinicschedulereportispopulatedwithalistofindividualswhoscreentobeeligible basedondateofbirthandresidence,whichareavailablefromthehospitalappointment schedulingsystem.SchedulereportsaregenerateddailyforHealthRegistryrecruiters, whousethisinformationtoapproachpatientsaroundthetimeoftheirappointment. Onceapproached,anindividualisinformedaboutthepurposeofthestudy,shownabrief videosummarizingthepurposeandscopeoftheHealthRegistry,andmadeawareof potentialrisks. Ifconsentisnotgiven,theindividual’sfinalstatuswillbesetas“Refused.”Iftheindividual isinterestedbuthasnotprovidedconsent,thestatusissetto“CheckBack”whichcanbe setto Abriefintakequestionnaireiscompletedduringtheconsentingvisit.Basicdemographic andcontactinformationisobtained,includingname,address,dateofbirth,gender,and race.Additionally,maritalstatus,employmentstatus,andinformationaboutthereferring physicianarerecorded. Toobtainthemostup‐to‐datecontactinformationforeachsubject,thisinformationis confirmedduringtelephoneinterviews. HealthRegistryrecruitersutilizecomputertabletsrunningMiFormssoftware(Mi‐Co, Durham,NC)torecordnotes,conducttheintakequestionnaire,andtoprocessconsent documentsignatures.Thetabletsareconnectedtoasecurewirelessnetwork,anddatais senttoadatabaseandfileserveroveranencryptednetworkconnection.Papercopiesofall consentdocumentsareused,filed,andback‐enteredintheeventofconnectivityissues. Section 3: Biospecimens UponenrollmentintotheHealthRegistry,asubjectmayprovidebiospecimenssuchas bloodortumortissue. Onoraftertheparticipant’sdateofconsent,bloodsamplesaredrawnbyaphlebotomist, loggedandcollectedbyhealthregistrystaff,andtransportedtotheUNCBiospecimen ProcessFacility.Bloodsamplesarenotcollectedforpartipantswhohaveaportacath installed.Subjectsmaychoosedelayorrefusetheblooddrawprocedure.Asaresult,the finalblooddrawstatusandnumberofapproachesarerecordedinthestudydatabase. AllblooddraweventsareloggedbyHealthRegistryrecruitmentstaffusingcomputer tabletsrunningMiFormssoftware.Participantsareassignedauniquebarcodenumber usedtotrackbloodsamples.Arecruitmentstaffmemberbringsthepatienttoa phlebotomysuitefortheblooddrawandgivesthephlebotomistbarcodedredand lavendertubevials.ThetimeofbloodcollectionisloggedinMiFormsandsamplesare temporarilyrefrigeratedon‐site.Withintwohoursofcollection,batchesofrefrigerated participantbloodsamplesaretransportedandloggedintotheBSPforfurtherprocessing, aliquoting,andbanking. Biospecimen Process Facility – Blood Samples Onceparticipantbloodsamplesaretakenfollowingconsentintothestudy,theyaresentto theUNCBiospecimenProcessFacility(BSP).Eachsampletakeniscollectedinatubewitha serialnumberlinkedtotheindividual.Samplesarebatched,packedinacooler,andwalked totheBSPlaboratorybyaHealthRegistrystaffmember(atripthatlasting5to10 minutes).OncethesamplesaredeliveredtotheBSP,theyareenteredintotheBSP laboratoryinformationmanagementsystem(LIMS)bythelaboratorytechnicianand HealthRegistrystaffmember. OncebloodsamplesaresignedintotheLIMS,BSPstaffareassignednewworkandapplya protocoltomeasure,aliquot,andstorechildsamples–thesequenceofwhichhasbeenpre‐ programmedintotheLIMS.AllprotocolstepsareproscribedbytheBSPLIMSsystem, whichprovidesaninterfacetoinputmeasurements,recordnotes,andtoassignchild samplecontaineridentificationnumbers. Childsamplesarebankedinfreezersintwoseparatelocationstoprovideafail‐safeagainst equipmentfailureorphysicalbreach,allowingsamplestobesecurelystored.Requeststo pullsamples(toperformadditionalprotocols,tomail,todestroy)arehandledby communicationbetweenHealthRegistrystaffandBSPtechnicians.Onceatechnicianis requestedtohandleasample,thedetailoftherequestislogged.Sample(s)areidentifiedin theLIMSsystem,pulledfromstorage,andpreparedaccordingtotherequest.A confirmationissentbacktoHealthRegistrystafftonotifythattherequesthasbeen completed. Tissue Procurement Facility – Tissue TheTissueProcurementFacilityisagroupsponsoredbyUNCLinebergerComprehensive CancerCenterandpartneroftheUNCHealthRegistrystudy.Astaffmemberfromthe TissueProcurementFacilityidentifies”targetable”surgicalproceduresscheduledamong consentedpatientsthatinvolvetumortissue.Intheeventthataresearchspecimencanbe saved,theTPFbanksthesampleforfutureuse. TPFstaffarepresenteachmorningandincludedocumentationforsurgicalstaffindicating patientconsentinastudyrequestingtissueforresearch.Aftersurgeryisperformed,TPF staffthentakecustodyoftissueandsenditontopathologyfortissueanalysis. Afterthepathologylabhassampledthetissue,anyremainderissenttotheTPFfor processingandbanking.Theprocessoftransportingasamplefromthesurgicalsuitetothe sample’sfinalbankingnormallytakesanhourorless. TheTPFusestwointerfacestoperformtheirwork.Scheduledsurgicalproceduresare cross‐referencedwithalistofconsentedsubjectsfromtheHealthRegistrystudy.Matching surgeryeventsareexaminedbystudystaffandplacedonatargetlist.Surgical appointmenttargetlistsareprintedforTPFstaffeachmorning. TheTPFLIMSsystemisusedtorecordinformationonanysamplescollected.Information includedintheLIMSsystemincludesspecimenID,bankingstatus,andnotesfromthe pathologyreport. Section 4: Questionnaires Interview‐baseddataiscollectedduringtheenrollmentprocessandsubsequentbaseline andfollow‐upinterviews. Limiteddemographicdataiscollectedatthetimeofenrollmentontotabletcomputers.The tabletsincludedatapre‐populatedfromtheCDW‐Hschedule.Theenrollment questionnaireprovidesanopportunitytocollectandconfirmbasicdataincludingname, dateofbirth,referringphysician,andcontactinformation. OnceanindividualisconsentedandenrolledintotheUNCHealthRegistry,subsequent questionnairedataisstoredinCDART–CarolinaDataAcquisitionandReportingTool–a web‐basedapplicationthatiswellsuitedforcomputer‐assistedtelephoneinterviewing (CATI). Thebaselinequestionnaireconsistsofacommonsetofinterviewelementscollectedofall subjectsshortlyafterconsent.Questionnaireelementscoverawideselectionoftopics includinghistoricheightandweight,exposuretoalcohol,qualityoflife,andaccessto healthcare. Annualfollow‐upconsistsofquestionnaireformsadministeredonanannualbasis. Enrollment Questionnaire Atthetimeofconsent,abriefenrollmentquestionnaireisadministeredtorecordbasic demographicdetailsincludingname,dateofbirth,gender,race,ethnicity,language, educationstatus,maritalstatus,referringphysicianinformationandcontactdetails.This questionnaireisadministeredbyconsentingstaffintheclinic.Questionnairedatais recordedoncomputertabletswithasecurewirelessconnectionandisstoredinastudy‐ maintaineddatabase. Baseline Questionnaire (CDART) Afterenrollmentintothestudy,subjectscompleteabaselinequestionnaireconsistingof morethan20constituentquestionnairesmeasuringhealth,symptoms,qualityoflife,and relatedvariables.Thesequestionnaireshavebeenvalidatedintheliteratureand underwenttestingandIRBapproval.Thebaselineinterviewlastsbetween45minutesto anhourandcanbecompletedovermultiplecalls. Afewofthequestionnairescontainskippatternsthatenableordisablefurtherquestions inasequencedependingonoutcome.Examplesincludeinformationonrateofalcohol consumption(dependentonansweringalifetimealcoholconsumption)inthealcohol informationformaswellasage‐basedskipsthatareutilizedinthehistoricheightand weightform(questionsrefertoheightandweightatages40,50,and60). Cancer‐Specific Questionnaires (CDART) Aseriesofcancer‐specificquestionnairesweredevelopedtocapturedataonspecific disease‐relatedpointsofinterestandareincludedinbaselineandfollow‐upquestionnaires administeredtostudyparticipants.ExampleareasincludeBreast,Prostate,Colorectal,and Hepatobiliarycancers. Assignmentofcancer‐specificquestionnairesoccursthroughanICD‐9billing‐codebased classification.TheresultsofthisclassificationappeartointerviewersinthePatient TrackingSystem.Amanualmethodofassignmentisalsospecifiedintheeventthatthe billingcodefeedfailstocorrectlyclassifyanindividual’sdisease. Annual Follow‐up (CDART) Aftercompletionofthebaselinequestionnaireandapplicablecancer‐specificquestionnaire forms,anannualfollow‐upinterviewservestocapturechangesinthisinformation,aswell asanysubsequentcancer‐specificinformationastheresultofnewdiagnoses. Section 5: Medical Records Abstraction Medicalrecordsinformationcomesfrommultiplesourcesystems.Billingcodedatafrom theCarolinaDataWarehouseforHealth(CDW‐H)isusedatthebeginningofenrollmentto assigncancer‐specificquestionnairesbasedonsubject‐specificICD‐9billingcodes. Atapproximatelythesametimethatanindividualvisitstheclinic,thehospitaltumor registrarbeginstorecordinformationfromasubject’smedicalrecordsinordertofulfill statecancer‐reportingrequirements.Thisdataiselectronicallystoredusingasoftware productcalledERS(ElectronicRegistrySystems,CincinnatiOH).Asdiagnostic,tumor staging,andcourseoftreatmentinformationbecomeavailable,thisinformationis abstractedintosoftwarethatcanformatstate‐compliantreports. TheUNCHealthRegistryStudypurchasedaninstanceoftheERSmedicalrecord abstractionsoftwareinordertoenablestafftoviewabstractedinformationonthesubset ofUNCHospitalpatientswhohaveconsentedtotheHealthRegistrystudyandenter additionalinformationontreatmentsreceived.(SeeHand‐Abstractionformore information). Finally,theSAS‐UNCpartnershipisworkingtodevelopingahealthoutcomesanalysistool basedusingasecuremedicalworkspaceconcept.ThistoolwilllinktoUNCHealthcaredata andenableresearcherstodiscoveranalyticcohortsandrunanalysesinasecured environment. CDW‐H Billing Codes – Cancer Specific Questionnaire Assignment Cancer‐specificquestionnaireassignmentisdrivenbyICD‐9billingcodesfromUNC Hospitalsbillingsystemsandservesasan“initialdiagnosis”untilmorespecificinformation isacquiredthroughpathologicdata.Arule‐basedalgorithmhasbeenimplementedto assignquestionnairesbasedonICD‐9billingcodes. SourcedataoriginatesfromCDW‐Hbillingcodereports.Thesereportscontainmedical recordnumber(MRN)correspondingtoeachsubject,thepatient’sdateofvisit,andICD‐9 code. CDW‐HDataSourcesUsedbytheBillingCode/QuestionnaireAssignmentAlgorithm HospitalPastDiagnosisReport Allhospital‐sidebillingdiagnosessince4/2009for patientswhowereseenataUNCcancerclinicin thelast14days P&APastDiagnosisReport AllPhysician/Associatesbillingdiagnosessince 4/2009forpatientswhowereseenataUNC Cancerclinicinthelast14days Thisdataisusedinconjunctionwithindividualdateofconsenttoselectthebillingrecords correspondingtothevisitclosesttothedateofconsent(thisisoften,butnotalwaysavisit onthesubject’sdateofconsent). Billingcodesfromtheselecteddateforeachpatientarematchedagainstaquestionnaire‐ mappingtable.Themappingtableidentifies220specificICD‐9codes. QuestionnaireassignmentsaredisplayedtointerviewersinthePatientTrackingSystemso thattheappropriateformsareselectedduringthetimeofinterview. Abstracted Medical Record Data Elements MedicalRecordinformationonconsentedpatientsconsistsofdemographicdata,tumorstaging information,treatmentinformation,andfollow‐upinformation.Thefollowingtablecontainsthe patientandcancer‐specificinformationforresearchpurposes. UNCCancerRegistryabstractedmedicalrecordvariables Demographics PatientUNCHRID Firstname Middlename Maidenname Lastname Nameprefix Namesuffix Dateofbirth Currentcounty Ethnicity Sex Race Tobaccohistory Familycancerhistory Alcoholhistory DiagnosisandStaging Sequenceoftheprimary Sitecode Topographycode Grade Histology Dateofdiagnosis Surgery Diagnosiszipcode Comorbidities Sitedescription Tumorsize Tumorextension/involvement Lymphnodeinvolvement Numberofpositivenodes Numberofnodesexamined Prostatetumorextension/involvement Pathologyreportnumber Primarypayer/insurance Survivalmonthssincediagnosis Tumorrecordnumber Generalstage AJCCstagebasis PathologicT PathologicN PathologicM PathologyAJCCstagegroup ClinicalTstage ClinicalNstage ClinicalAJCCstagegroup Clinicalstagedby TNMeditionnumber Justificationforclinicalstagingelements Justificationforpathologicstagingelements Generalstagetext Typeofsourcedocuments Diagnosiscomments Operativefindings Comments Surgerydate Surgerytype Scopeoflymphnodesurgery Lymphnoderemoved Surgeryofregionalsites Firstorsubsequentsurgery Treatinghospitalcode Treatment Recurrence Other Treatmentdate Regionaltreatmentmodality Boosttreatmentmodality Chemotherapy Hormone/steroidtherapy Immunotherapy Hematologictransplant/endocrineprocedure Othertreatment Palliativeprocedure Firstorsubsequenttreatment Treatinghospitalcode Recurrencedate Recurrencetype Recurrencemetastasissite Cancerstatus Patientstatus Dateoflastcontact Follow‐upmethod Cancerstatus Patientstatus Dateoflastcontact Follow‐upmethod Medical Record Hand‐Abstraction AsetoffieldsiscreatedintheERSsystemtodetailinformationonfirstcourseoftreatment forastudysubject.ThesefieldsareenteredbyUNCHR/CSCstaffandappendedtotheERS record. Hand‐abstractedfieldsincludeavariabletosignifywhetherfirstcourseoftreatmentwas performedoutsideoftheUNCcancerhospital.Inaportionofthosecases,documentation fromoutsideclinicsarescannedandreceivedbythehospitaltumorregistrarandare availableforenumerationoftreatments. Becausefirstcourseoftreatmentwillvarybycancersiteandotherindividualfactors,the detailofeachrecordwillvary.Theavailabilityofinformationforanindividual’streatment willinfluencethecompletenessofthesehand‐abstractedfields.Inmanycases,this additionalabstractionwillserveasabasistovalidatetreatmentinformationfoundinother sectionsoftheERSrecord. Hormone,immunotherapy,andchemotherapyagentsinvolvedinthefirstcourseof therapyarenotedinappropriatesectionsofthefreefields.Abestestimateoftreatment startdateisrecordedbasedonrecords.Thisestimateisbasedonrecordof dispensing/administrationwithinvisitnotes.Eachagent’sNSC(NCINationalService Center)numberisrecorded.Often,coursesoftreatmentconsistofregimens.Fora particulardrugregimen,multipledrugsmaybeadministered,eachwithit’sownNSC number.Eachdrugintheregimenisrecorded. Treatmentcompletionstatusisrecordedandcorrespondstoreasonsforinterruptionor suspensionoftreatment.Successfulcompletionandunknowncompletionstatusarealso recordedinthisfield. UNCHR/CRCabstractedmedicalrecordsvariables* ChemoAgent1‐6** ChemoAgentNSC StartDate Enddate NumberofCycles Cycleduration Completionstatus HormoneAgent1 Startdate HormoneAgentNSC ImmunotherapyAgent1 Startdate ImmunotherapyAgentNSC Other TreatmentsOutsideofUNC(Binary) DateofHRabstraction *ERSfreedatafieldsmodifiedtoincludethoselistedinthistable **Datawillbeabstractedformultipletreatmentswhennecessary(1,2,etc) Appendix 1. System‐Specific Information Patient Tracking System TheShepsIntegratedResearchSystem(“SIRS”)isasecure,enterprisedatabaseand programmingframeworkspecificallydesignedtomeettheneedsofhealthresearch projectsattheCecilG.ShepsCenteratUNCChapelHill(“Sheps”).SIRSprovidesreusable modulesfordatacollection,management,andtrackingforadiversesetofstudies, registries,andresearchcoordinatingunits.SIRSisspecificallydesignedtoprovidea frameworkforprogrammingthatsimplifiescommonprogrammingtasksandallows customizationwhilemeetingapplicablesecurityrequirements.TheSIRSframeworkis completelywebbasedandopensourceutilizingMySQL,Apache,JavaScriptandPHP. TheShepsIntegratedResearchSystemoffersmanyadvantagestoinvestigators • Security • Datamanagementexpertise • InputandfeedbackfromexperiencedSIRSprogrammers • Abilitytoincorporatedesignsfrompreviousstudies • Continuitywithinprojectsbutacrossprojectsovertime • Faster“intothefield”capability • Lowercost • Availabilityofcommoncomponentswithtestedandverifiedcode • Thoroughdataauditing Allsystemloginproceduresanddatasubmissions(e.g.,fromstudystafforsurvey respondentsthroughtheInternet)areencryptedviatheSecureSocketsLayer(SSL) protocoltoasecurecentraldatabaseattheShepsCenter.User‐levelpermissionsarebased onuserrolesandaredefinedwithintheprojectsystemtolimiteachuser’saccesstoonly thoserecordstheyareauthorizedtosee. Thecentraldatabaseforprojectsrunsonamirroredserversystemwithautomaticfail‐ overfeatures,dailybackupsandtransactionlogs.ThissystemisphysicallylocatedinaTier IIDataCenterprovidingbackuppowersources,climatecontrol,fireprotectionand24x7 surveillance. Auditlogsarereviewedroutinelytoverifysecuritymeasuresareoperational.Theservers arescannedweeklyforvulnerabilitiesandarecurrentlymaintainedatthehighestlevelof vendorandCERTsecurityrecommendations.Dataareneversharedoutsidetheproject unlessauthorizedbytheprojectleader.Userauthenticationisbasedonuserpasswords. Passwordcreationrequirementsareinplacetoguarantee“strongpasswords”asdefined bytheCERTsecurityrecommendations.TheleadsystemsadministratorisGIACSecurity EssentialscertifiedthroughMay,2014. TheUNCShepsCenterendeavorstopreservetheprivacy,confidentiality,andsecurityof protectedhealthinformationthatmaybepartofhealthrecordsorresearchdatasets. ProtectedHealthInformation(PHI)ishandledaccordingtoappropriateHealthInsurance PortabilityandAccountabilityActof1996(HIPAA)PrivacyandSecurityRegulations.Sheps Centerprogrammersandresearchstaffwhoworkwithsensitivedataarerequiredto completeappropriateHIPAAtrainingwithperiodicupdates,completeShepsCenter internaltraining,complywiththeUNCITSecurityPolicies,andagreetotheprovisionsof theShepsCenter’sRulesofBehaviorandSanctionPolicy.TheShepsCenterstrivesto implementreasonablesecuritycontrolsguidedbyFISMA,HIPAA,andOMBCircularA‐130, AppendixIII. Overview of BSP LIMS Quality Assurance / Quality Control The Biospecimen Process Facility (BSP) Laboratory Information Management System (LIMS)usesOracleasadatarepository.Therearethreedatabaseshostedontwoservers supportedbyInstructional&InformationSystems,UNCSchoolofPublicHealth.Backups occur on both servers on a daily basis. As the need arises, snapshots of the production database are copied to the two additional databases (staging and development). In the unlikelyeventofdatacorruptionontheproductionserver,theSchoolofPublicHealthwill beabletorestorethesystemfromthelatestbackup. Thepurposeofthestagingdatabaseistoprovideatestenvironmentforapplicationcode priortoitsreleaseintothelaboratoryenvironment.WiththeuseofcustomSQLscripts,it ispossibletorapidlysetupamirrorimageoftheproductiondatabase.Thisisusefulfor rapidresponsetoLIMSmaintenanceissues.Userscanreportbugsbysendinganemailto informaticshelp@unc.edu.ThiswillcreateahelprequestintheLinebergerBioinformatics groupticketsystem.Applicationcoderunningagainstthestagingdatabaseisalwaysfound inthehighestnumberedbranchwithinthecodeversioningsystem. Thedevelopmentdatabaseisalsoperiodicallymirroredfromproductionbutwithpossible schemamodifications.Thisdatabaseprovidesadataenvironmentformajorcodechanges, whichsometimescontinueoveraperiodofmonths.Applicationcoderunningagainstthe development database will always be found in the HEAD branch of the code versioning system. LIMS code development is done using the Eclipse software development tool. With few exceptions, aspects of the LIMS application (Java source code, SQL scripts, database packages,helpdocumentation,etc.)aremaintainedwithinEclipseandallofthesefilesare backedupinacodeversioningsystemonbioinfostore.unc.edu.Therearetwobranchesof codedevelopment:HEADandBranch_X,where Xrepresentsthebase‐versionnumberof thelatest,orhighestrelease.Atthetimeofwritingthisdocumentthelatestreleaseis11, e.g.Branch_11isthecurrentbranch. Before releasing a new version of the LIMS, we conduct unit and integration testing. During unit tests, developers verify that the newly added code functions properly and solves reported bugs. Integration testing is used to make sure the changes don’t break existingfunctionality.Wehaveaseriesofgeneraltestcasesthatwerunbeforereleasinga new version. The steps for deploying a new version are documented and stored in our group’sinternaldirectory.Weareimplementingcodereviewsasapartofthedeployment process. Eachreleaseistaggedwithaversionnumber.Thecodeversioningsystem(CVS)maintains a history of the code versions and a change history for each file in the repository. From Eclipse,youcanviewthechangehistoryforagivenfileandcompareittoanotherversion. Wedocumentthechangesineachreleaseonourgroupwiki. WhennewstudiesareaddedtoLIMS,theBSPlabmanagersmeetwiththeprincipal investigatortodiscussthesampleprocessingworkflow.Then,theBSPlabmanagerscreate protocolswithintheLIMStostandardizetheproceduresineachstepoftheworkflow. Additionally,eachlabtechnicianreceivesperiodictrainingtolearnthelab’sstandard operatingproceduresaswellastomaintaincertificationspertinenttotheworkinthelab (iebloodbornepathogen,HIPAA,andCITItraining).TheLIMShasthefunctionalityto maintainalistingofthecertificationsandvaliditydatesforeachuser.TheLIMSalsohas thefunctionalitytotrackproject‐specificIRBcertifications. Onamonthlybasis,theBSPlabmanagersgeneratecheck‐inreportsfromLIMStoverify thevalidityofsamplecollectionanddrop‐offdates.IntheLIMSprojectsetup,thereisan optiontosendcheck‐inreportstostudystaffandlabmanagersonaweeklyordailybasis. Thereisascheduledtaskthatrunsdailyandemailsthereporttoregisteredusers.This helpsthestudystaffandlabvalidatewhatsamplesweresentandreceivedeachweek. TheLIMSmaintainsanaudittrailforeachsampleprocessedinthesystem.Eachaudit recordcontainsthetechniciansnameandadateandtimestamp.Theaudittrailtracks everythingthatisdonetothesamplefromthetimeitwascheckedintothesystemtowhen itwasdiscardedorshippedtoanotherfacility.Thereareauditsforsamplecheck‐in, storageassignment,extractions,openandclosingofprotocols,discards,planchanges,etc. TheLIMSusesseveraldifferenttypesofinputfieldsontheinterfacedependingonthetype ofdatabeingentered.Fornumericvaluessuchasvolumeandconcentration,theLIMS displaysaninputfieldthatallowstheusertoselectanumberfromanorderedlist.There areupanddownarrowsnexttothedatafieldforsteppingthroughthevaluesinthe sequence.TheLIMSusescheckboxesforyesandnofields.Forexample,tomarkasample asdiscarded,theusercancheckthediscardbox.Dropdownboxesareusedtoselectvalues likeunits,containertypes,andprojectnames.Inputfieldsforcomments,participantids, dropoffcourier,etcarefreetext. TheLIMSprovidesdataqualityassuranceandqualitycontrolbyvalidatingdataentered intothesystem.Forexample,OpticalDensitymeasurementsaretakenontheNanodrop andtheDropSense.Theequipmentsavestheopticaldensitymeasurementsand concentrationstoafile.WhenthatfileisloadedintotheLIMS,thesystemwillverifythat thedataisnumeric.Ifit’snot,theLIMSwilldisplayanerrormessagetotheuser.Ifa donorcodeformatisdefinedinaprojectcheck‐inprotocol,theLIMSwillchecktoseethat theenteredtextfitsthedesiredformat.Theuserwillnotbeabletocheck‐inthesample untilhe/sheentersaparticipantidinthecorrectformat.Eachprotocolcandefinecertain fieldsasrequired.Whenprocessingsamplesthroughaprotocol,techniciansaren’tableto completeaworksetuntiltheyhaveentereddataintoallrequiredfields.Thesearejusta coupleexamplesofcaseswheretheLIMSvalidatesuserinput. BioSpecimen Facility Information Technologies (LIMS) TheBSPutilizesastate‐of‐the‐artspecimentrackingsystemdesignedspecificallytomeet theimmediate,inventory‐styletrackingneedsofmultiplehealthresearchprojects.Itis referredtoastheLIMS(LaboratoryInformationManagementSystem).TheLIMShasbeen designedtobeflexibleandextendibleforfutureneeds.Allsamplesenteringthelabreceive 2Dbarcodelabelsthatallowustofollowanysample’sprogressthroughthespecific proceduresindicatedbytheappropriatestudyprotocol.Samplesthatenterthelabare givenaBSPIDnumber,furtherprotectingastudysubject’srights.Theselabelsalsocontain ahumanreadableportionandadditionalstudyencodedIDinformation. TheBioSpecimenProcessingFacilityLIMSisOracle‐basedandmaintainedbytheSchoolof PublicHealthwithsecurityandbackup.Theuserinterface(developedandmaintainedby theSchoolofMedicine)isimplementedasaJavathick‐clientwithlimited(readonly)WEB accessprovidedtoprincipleinvestigatorsandtheirstaff.Thethick‐clienttrackscreation, storage,movement,anddiscardingofcontainers(vialsandplates)andthespecificsof containercontents(materialtype,volume,concentration,techniciancomments,etc.)andis accessedonlybyBSPFacilitystaff.Allcontainershaveastudycontext.BSPstaffhasaccess toallstudiesbutonlyspecificPIstaff(assetupwithinthesystem)canaccessinformation associatedwiththeirprojectviatheWEBclient. LIMSusersarerequiredtologinusingtheiruseridandpassword.Thepasswordsmustbe atleast8charactersandmustcontainanumberandaspecialcharacter(!,@,#,etc).The LIMSwillnotallowuserstore‐usetheirlasttwopasswords.Eachuserisassignedarole, whichdefineswhatfeaturesareavailabletothem.Inadditiontoroles,PIstaffmembers areassociatedwithprojects.StaffmemberscanlogintotheWEBclienttoviewreportsfor samplesintheirprojects. EachcontainercreatedbythesystemisassignedaBSPidentifierthatisunique‐ineffect, thisisthefacilityassetidentifierforthatcontainer/sample.Eachcontainerislabeledwith theBSPidentifier,project/donoridentifiers,typeofcontainedmaterial,volume, concentration(ifapplicable),dateofcreation,andcurrentstoragelocation.Containersmay bepre‐assignedtoaprotocolpathwhicheventuallyleadstothedepartureofthe containersfromthefacility,butmayalsoresultinlong‐termstoragewithinthe facility.Throughaqueryinterface,setsofcontainersmaybeidentified,pulled,andbe furtherprocessedwithinthefacilityorbeshippedtootherfacilities. Anaudittrailismaintainedoncontainersandcontent.Thistrailrecordssuchthingsas whenandwhodropsoffcontainerstotheBSP,whenthecontainerwascreatedasitmoves throughprocessingintheBSPasdirectedbythestudiesprotocols,whichtechnician createdit,whenandwhereitwasstored,whenandwhereitwaspulledfrom,etc.The systemwilltrackmaterialsthataretransferredtootherfacilitiesorPIcollaboratorsas well. TheLIMShasthecapabilityofacceptingprocessinglogsgeneratedbytheAutopureLS (DNAextractonrobot)andtheMultiprobeII(aliquotingrobot).Theselogscanbe transferredtotheLIMSatthecompletionofeachrun.Theselogsarelinkedtothe individualsampleshistoriesandcanbereferredtointhefutureforavarietyofreasons. TheresultsfromanalysisdonewithinthefacilityarerecordedintheLIMSdatabase.This includesagarosegelanalysis(withimage),opticaldensity(withwavegraph),real‐time PCRandbioanalyzerresults.Analysisreportsareavailabletoboththefacilitystaffand projectstaff(throughtheWebinterface).Thecurrentinventoryofagivenprojectisalso availableasareport.Thisshowstheentireprojecthistoryintermsofmaterialthatwas checkedintothefacility,createdbythefacility,andshippedfromthefacility. NoPersonalHealthInformation(PHI)ismaintainedanywhereintheBSPsystems.When donorsamplesarecheckedintothefacilitythesystemallowsforlimitingtheuseofthe samplesbasedupondonorpreferences(i.e.allowgeneticresearch,destroyatproject completion,orrestrictresearchtooriginalproject). Onadailybasis,theLinebergerDatawarehouseandBiospecimensRepository(LDBR) loadsLIMSproductiondataforreporting.Thedatawarehouseusesaread‐onlyaccountto connecttotheLIMSdatabase.StoringLIMSdatainthedatawarehouseallowstheHealth Registrystafftocreatereportsfortheirsamples.Thesereportsincludeinformationabout thesamplesthathavebeencheckedin,thesampleinventory,andnucleicacidanalysis data. Future TPF LIMS System DevelopmentofthefutureTPFLIMSSystemwillbebasedontheBSPLIMSsystemandwill besimilarinscope,development,andimplementation.TheFutureTPFLIMSsystemwill storeinformationoncollectedtissue,pathologystatus,sampleprocessingprotocolsand methods,andbankingandinventoryinformation. Electronic Registry System (ERS) ElectronicRegistrySystem(ERS)isaCancerRegistrysoftwaretoolthatincludesthe standarddatasetrequiredbytheCommissiononCancer(CoC)andmeetsthe requirementsoftheNorthAmericanAssociationofCentralCancerRegistries(NAACCR). TheUNCCancerRegistry’sCertifiedTumorRegistrarsuseERSasadatacollectiontoolfor manualelectronicmedicalrecordsabstraction–requiredbystatelaw.Approximately 80%ofthehospitalsinNorthCarolinauseERS. TheERSsoftwaretoolfortheUNCCancerRegistryismaintainedandhostedbyERSand deliveredasavirtualizeddesktop.Itisaccessedviawebsiteandrequiresentryof credentials.TheUNCHealthRegistry/CancerSurvivorshipCohort(HR/CRC)purchased theERSsoftwaretooltofacilitatetransferofUNCCancerRegistrydatadirectlytoHR/CRC viaanERSdevelopedsoftwarepatch.TheUNCHR/CRCERSwillbemanagedbythe LinebergerDataWarehouseandHR/CSCITteamandERSprogrammingsupportgroupin conjunctionwithISDtoassureversioningcomparability.InadditiontotherequiredCoC datasets(seeTable1),ERSmakesavailabletotheUNCHR/CSCotherdatafields,including thosethatcanbecustomized,tofitourspecificneeds.Theadditionalfieldsinclude expandedresearchanddiagnosticfields,clinicaltrialfieldsaswellasuserdefinedfields thatcanbecreatedandmaintainedbytheuser.TheHR/CRCstaffwillmanuallyabstract theseadditionaldatafields(seeTable2)fromtheelectronicmedicalrecordtocomplement thedatathatisprovideddirectlyinERSfromtheUNCCancerRegistry.Codingmanualsare onlineandmaintainedbytheERSsoftwarecompany.ERSprovidesuserswithavery extensivereportingmodulefordataanalysistocomparetreatmentanalysis,survival, incidencebysite,stage,race,etc.Anydataiteminthesoftwarecanbeselectedandusedfor reportingpurposes.Thesoftwarecontainsafollowupmodulethatallowstheuserto automaticallyschedulefollowuplistsandletterswithpatients. ERSprovidesthreedaysofinitialon‐sitetrainingfornewusersaswellasunlimitedonline training.AcompleteusermanualisprovidedaswellasaVideoLibraryoftrainingtutorials (seeonlineResourcelistbelow).Thesoftwareisupdatedquarterly(ERSnotifiesISDor userviaemailthatthesoftwareupdateanddocumentdetailingupdatechangesis available)andquarterlytrainingwebinarsareprovidedthatareawardedcontinuing educationcreditsfromtheNationalCancerRegistrarsAssociation(NCRA).ERSprovides unlimitedsupporttousersforallregistryandtechnicalissues. TobeaCTR(CertifiedTumorRegistrar),oneisrequiredtohaveaminimumofa2year degreeinahealthrelatedfieldandpassthenationalCTRtest.Asof2012,eachregistrar mustbecertifiedtoperformabstraction.Thereareinternaleditcheckswithinthesoftware thatcomeupifillogicalinformationisentered,suchasfemaleforprostatecancer,zipcode andcountycodematchingerrorsaswellasprocedureandstagingconflicts,suchas enteringpathologicstagingwhenthepatienthashadneoadjuvanttherapy.Requiredfields cannotbeleftblank.Additionally,about10%ofthecasesareidentifiedbytheUNCCancer Registrarandarereabstractedtocheckforaccuracy.Aqualitycontrolprotocolinvolving reabstractionofaproportionofrecordstomonitordataqualityofadditionalHR/CSC abstracteddataelementswillbeimplemented.Additionally,bothUNCCancerRegistryand UNCHR/CSCmanuallyabstractedmedicalrecordsdataelementswillbecomparedwith plannedEMRextractionsforadditionallyqualityassessment. Resources: 1. ERSWebsite http://www.ers‐can.com/ 2. FORDSmanualfor2013 http://www.facs.org/cancer/coc/fords/fords‐manual‐2013.pdf 3. 7theditionAJCCstagingmanual: http://www.cancerstaging.org/products/ajccproducts.html ISBN:978‐0‐387‐88440‐0(mustpurchasefor$65–seewebsite) Appendix 2. System‐Specific Data Mappings CPR‐OR Tissue Collection Tracking TheUNCHealthRegistryTPFReportcontainstissuebankingstatusinformationthatis reportedincoarsergranularitybasedonseveralspecificbankingstatuscategories.This tableexplainsthescenarioswheretissuesarenotcollected. Status Banked After Hours Surgery Stopped (updated from Aborted) Completely Submitted to Path Canceled Improper Consent Explanation Tissue was received and processed Cases that run past 5:30pm Monday through Friday. Cases are then targeted the next morning before they are put on formalin by pathology (with the exception Friday cases, after hours cases will be updated the next day) Surgery was stopped (this generally occurs when frozen sections from complex surgery cases show metastatic disease, and the surgeon decides that the patient is better off without continuation of surgery) Cases in which tissue procurement is not allowed to take any tissue because all of the tissue is needed by pathology (examples include: lymphoma workups, spleens submitted to hemepath, medical kidneys, uterus cases with complex atypical hyperplasia, BRCA ovaries) Cases that were on the schedule but were either cancelled or moved to another date Cases in which HIPAA was not signed, the consent form was not signed, dates were invalid, or surgeon did not consent patient prior to surgery Tissue Status TISSUE COLLECTED Temporary status due to pathology hours. On TPF Report Final status if collected on a Friday. NO TISSUE COLLECTED NO TISSUE COLLECTED “Not Enough Tissue” (Sample sent to Surg Path) NO TISSUE COLLECTED TISSUE NOT COLLECTED Infectious Margins Biopsies Too Small No Tumor Seen Not Targetable Procedure No Consent Withdraw Case that are known to be infected with HIV, HBV, HCV, or TB are not banked by TPF Wide local excision (WLE) melanomas or breast re-operative cases in which margins were previously positive are not banked by TPF Scope cases which produce little or no tissue are not banked by TPF TISSUE NOT COLLECTED TISSUE NOT COLLECTED “Not Enough Tissue” (Sample sent to Surg Path) TISSUE NOT COLLECTED “Not Enough Tissue” Cases in which the PA can see tumor, but there is not enough tissue to be given to TPF TISSUE NOT COLLECTED (Sample sent to Surg Path) “Not Enough Tissue” - Cases in which there is either no cancer diagnosis, or the tumor cannot be seen or palpated (examples include: abnormal mammograms, benign disease cases, and cases with only normal tissue) are not banked by TPF Cases that will not produce tissue Cases that blank consent form is found in the chart (recently updated) Cases that subject revoked the consent signed prior the surgery (recently updated) TISSUE NOT COLLECTED (Sample sent to Surg Path) “No Tissue” (No Sample Sent to Surg Path) TISSUE NOT COLLECTED TISSUE NOT COLLECTED TISSUE NOT COLLECTED